Unsolved Mysteries: After Four Decades, Daniel Drucker, MD, Is Still Unlocking Scientific Secrets
By Glenda Fauntleroy Shaw
Nov 2024
The Endocrine Society’s 2025 Fred Conrad Koch Lifetime Achievement Award recipient, Daniel Drucker, MD, first discovered his passion for science in high school when he learned “this is how stuff works.” He’s still learning to this day, and he tells Endocrine News about his ongoing scientific quests, the mentors who made a difference along the way, and why even old ideas are still valid.
Daniel Drucker, MD, knows the enormous impact his discoveries have made to lives of those living with diabetes and obesity, but after 40 years of scientific research, he believes there’s still more mysteries for him to unlock.
Drucker, the 2025 recipient of the Endocrine Society’s Fred Conrad Koch Lifetime Achievement Award, is a professor of medicine at the Lunenfeld Tanenbaum Research Institute of Mt. Sinai Hospital and the University of Toronto in Toronto, Canada, is recognized for his ground-breaking contributions to the understanding of the physiology and pharmacology of glucagon-like peptides (GLPs) and their use for the benefit of patients. His discoveries of GLP-1, GLP-2, and dipeptidyl peptidase-4 (DPP-4) activity provide the foundation for the some of the largest sectors of drugs for obesity, gut disorders, and type 2 diabetes.
From ENDO 2018 in Chicago, Ill., Drucker (center) is pictured with Patricia Brubaker, PhD, from the University of Toronto (left), and 2018 Endocrine Society President Susan Mandel, MD, MPH.
His spark for science was first ignited in high school after Drucker – born to European immigrants in Montreal, Canada – and his family moved to Ottawa when he was 13 years old.
“It just sort of appealed to me, the fact there were laws governing scientific processes, whether it was in physics or chemistry, that one can explain how stuff happens, and I think that was very attractive to me,” he recalls. “Maybe I was insecure in my ability to deal with the humanities and English literature and more abstract processes, whereas the science was ‘this is how stuff works.’”
Drucker received his medical degree from the University of Toronto and later took a research fellowship position at the Massachusetts General Hospital lab of another renowned endocrinologist, Joel Habener, MD. Habener, too, has played a pivotal role in the early discovery of GLP hormones.
Life is Often Full Circle
Habener’s lab was a very interesting place, Drucker recalls.
“It was very well funded at the time, with multiple NIH grants and funding from Howard Hughes,” he says. “That was really a luxury, in that we didn’t have to worry every day about where can we get the money to buy this, or can we possibly afford to do the next experiment?”
“It was a wonderful environment because there were some really smart people from all over the world who were attracted to Mass General and to Harvard and certainly, to Joel’s lab, and I think that was really important because you went to work every day, and there’s so many other people surrounding you who have great ideas and who are worth listening to and are role models themselves,” Drucker says. “That was the environment that I found myself in, and Joel was an ideas person.”
“It was a little intimidating for me,” Drucker continues. “I didn’t have a strong scientific background, and to be honest, I didn’t really know what I was doing the first few months, but it was a great place to learn, and that’s where I had the opportunity to learn science.”
September 18, 2023 – Photos of Daniel Drucker taken at Mount Sinai Hospital (photo by Polina Teif)
“It’s the most exciting time yet to be doing science related to GLP-1. So, it’s quite a privilege, to be honest, to be working in a field that has remained so fresh and so exciting for so many years. You really don’t see that that often in biomedical science.”
Who could have guessed the two of them would come together years later on the GLP-1 discovery?
“That’s the thing about basic science,” he says. “It sometimes literally will take a decade or even longer, to become apparent what the real relevance and potential is. Back in those days, none of us foresaw the current landscape with regard to obesity. We thought GLP-1 might be useful as a diabetes treatment, and after 15 or 20 years, that turned out to be the case, but I think the obesity story was not really apparent to anybody in the 1980s. That came much later.”
Biggest Health Story of 2024?
While scientists may have been aware of the possibilities in the late 80s that GLP-1 could do more than treat diabetes, for the mainstream public, Ozempic and Wegovy seem to hit the news in 2024 like a lightening bolt.
“In 1996, there were three papers published that showed that GLP-1 inhibited food intake, and one of them was from my lab in Toronto,” he explains. “So, we had a sense that here’s something that not only lowers blood sugar for diabetes, but also reduces food intake, and then it took 18 years from 1996 to 2014, to when the world’s first GLP-1 medicine was approved for the treatment of obesity.”
The first drug approved in 2014 was liraglutide, but liraglutide didn’t become the topic of conversation at everyone’s dinner table and didn’t take the social media by storm, recalls Drucker. “The turning point was once we got semaglutide for the treatment of obesity, which really showed the potential for GLP-1 to produce much more profound weight loss than we’d seen before.” Drucker says that for researchers in the specialty, GLP-1 medicines are like a gift that keeps on giving.
Members of the Drucker Lab (from left to right): Eloisa DaSilva, Susanna Fang, Dianne Matthews (seated), Rui Shang, Rola Hammoud, Maria Gonzalez, Daniel Drucker, Fiona Cui (seated), Kyle Medak, Xiemin Cao, Jacqueline Koehler, Bernardo Yusta (seated), Chi Kin Wong, and Wenran Ren.
“We started with type 2 diabetes, and then we moved to obesity,” he says. “Then we got really good data showing that GLP-1 reduces heart disease and strokes, and more recently, we have very exciting data showing that it reduces kidney disease and severity of sleep apnea. And it’s now in clinical trials for metabolic liver disease, peripheral artery disease, Parkinson’s disease, and for Alzheimer’s disease.”
“It’s the most exciting time yet to be doing science related to GLP-1,” he adds. “So, it’s quite a privilege, to be honest, to be working in a field that has remained so fresh and so exciting for so many years. You really don’t see that that often in biomedical science.”
But has there been an enormous branding fail in marketing GLP-1 as a weight loss drug? Did scientists finally discover the drug that cures obesity, only to have people ashamed to admit using it? Why are overweight and obese people still being called “cheaters” for not just exercising and dieting to lose weight?
“There’s clearly a stigma surrounding obesity that we don’t see with many other chronic medical conditions, and I think many folks, including, healthcare professionals and scientists, harbor the opinion that you should be able to control your own body weight, and it’s a moral failing or a lack of discipline,” Drucker says. “We tend to make judgements about someone’s inability to lose weight, even though there’s an abundance of evidence and science that shows that obesity is a disease, and your brain becomes wired differently.”
“That’s the thing about basic science. It sometimes literally will take a decade or even longer, to become apparent what the real relevance and potential is. Back in those days, none of us foresaw the current landscape with regard to obesity. We thought GLP-1 might be useful as a diabetes treatment, and after 15 or 20 years, that turned out to be the case, but I think the obesity story was not really apparent to anybody in the 1980s. That came much later.”
Obesity fights a person’s attempts to lose weight, Drucker adds, and many people are not willing to acknowledge that.
“We would never say to someone with Crohn’s disease, or arthritis, with a horrible infection ‘why can’t you just get better yourself?’” he emphasizes. “People would be appalled if you said that, but for some reason, it tends to be what some segments of society do say when confronted with this challenge surrounding weight loss.”
“With the GLP-1 medicines, many people can lose 10%, 15%, 20%, or more of their weight, and they can proudly look at their colleagues, their family members, and people who may have been questioning them and say, ‘you see, I just needed help.’”
For people needing the GLP-1 weight loss drugs, however, a large barrier to access is the drugs’ high cost, but Drucker says changes are on the horizon.
Drucker (far right) grabbing coffee with his sons, Aaron, Jeremy, and Mitch while the family was in Jerusalem where Drucker received the 2023 Wolf Prize in Medicine “for pioneering work in elucidating the mechanisms and therapeutic potential of enteroendocrine hormones.”
“I have no doubt that the medicines will become much more affordable, and there’s several reasons why,” he says. “First, there will be competition with many new types of GLP-1 medicines, and some of them will be pills that are much easier and cheaper to make, so that alone will bring down the cost of the medicine.”
“Also, right now, we have Novo Nordisk and Eli Lilly and no one else,” Drucker continues. “But in five years, there’s going to be a half a dozen other companies involved that will also bring pressure on the price. Then we also have Congress, which is examining the prices of medicines and asking Medicare and Medicaid to look carefully at negotiating price discounts. In September, the CEO of Novo Nordisk said that he believes that Ozempic will be the subject of price discounts mandated by Medicare/Medicaid negotiations in a couple of years.”
During a September session before the Senate Committee on Health, Education, Labor and Pensions, the CEO of Novo Nordisk indeed faced tough questions about the high prices for its drugs Ozempic and Wegovy. A report issued by the Committee showed the cost of Wegovy is significantly less in European countries — from $140 a month in Germany to $92 a month in the United Kingdom. Americans pay about $1,349 a month for the exact same drug. According to news reports of the Senate hearing, Novo Nordisk CEO Lars Fruergaard Jorgensen agreed to meet with pharmacy benefit managers to discuss lowering the costs of the two drugs.
Grandkids and Golf?
Drucker says that there are days when he thinks that after 40 years of scientific research, maybe it’s time to just play more golf and spend more time with his grandchildren. But he laughs and says he does plenty of both already and there’s still time left to spend in the lab.
So, what’s his next scientific mystery to uncover?
“This may sound silly, but we really work on the same things today that we would’ve worked on 10 or 15 years ago, which is how do these GLP hormones work?”
“In 1996, there were three papers published that showed that GLP-1 inhibited food intake, and one of them was from my lab in Toronto. So, we had a sense that here’s something that not only lowers blood sugar for diabetes, but also reduces food intake, and then it took 18 years from 1996 to 2014, to when the world’s first GLP-1 medicine was approved for the treatment of obesity.”
“We know GLP-1 does all these really cool things, but we don’t really understand how. You know, there’s a new medicine tirzepatide, or Mounjaro, and it’s just fantastic, developed by Eli Lilly, and it activates both GLP-1 and GIP, but we don’t completely understand how that works.”
Drucker says in his basic science lab they use molecular and cellular biology and mouse genetics to be able to ask these questions: How is this medicine working? Where is it working? Which cell types is it targeting? How does that magic happen?”
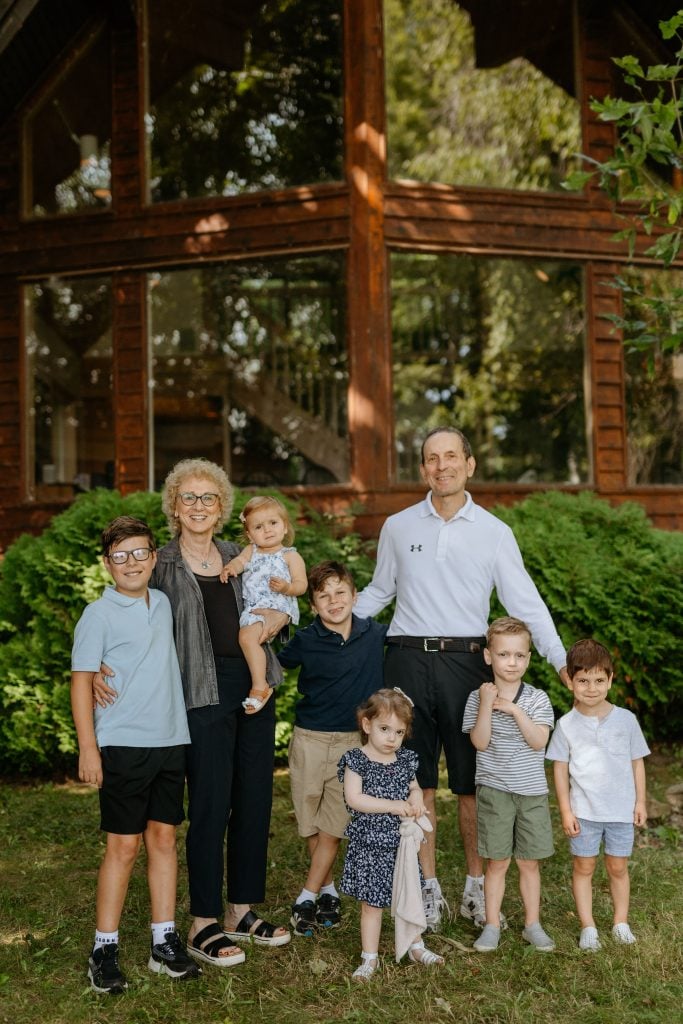
Drucker, his wife Cheryl Rosen Drucker, and their grandchildren, Benjamin, Madeline, Miles, Hallie, Brendan, and Kyle.
But Drucker says he hears the criticisms from some who say he’s been doing the same research for decades and questions why he doesn’t have any new ideas.
“That’s a valid criticism,” he acknowledges. “But for me, to see all of these fantastic new trials showing benefits in people, I really still want to understand how these medicines work.”
Shaw is a freelance writer based in Carmel, IN. She is a regular contributor to Endocrine News and writes the monthly Laboratory Notes column.
For the eleventh year running, Endocrine News talks to editors from Endocrine Society publications to unearth the most impressive breakthroughs in endocrine science and research for 2025. From GLP-1s, adrenal treatments, and acromegaly breakthroughs to obesity, diabetes, and cutting-edge research in reproductive medicine, 2025 was a banner year for endocrine research and researchers! For more…
New research shows that that the diabetes/obesity medication tirzepatide can cause clinically meaningful improvements in blood sugar control and weight loss in children and adolescents with type 2 diabetes aged 10-17 years whose diabetes and weight are inadequately controlled with an existing treatment regimen of metformin, insulin, or both. The study (the SURPASS-PEDS trial), led…